National Stroke Awareness Month:
Tips on Stroke Rehab and Identifying Risk Factors
By: Erica Pitsch, PT, DPT, NCS

Part 1: Risk Factors and signs of stroke
By the numbers: According to the CDC, “stroke is the 5th largest cause of death and is the leading cause of severe disability”. Early medical attention can dramatically change the outcome of a person having stroke, so educating our patients on risk factors and recognizing signs of stroke is essential.
Risk Screening: We often review a patient’s medical history. When we see diabetes, high cholesterol, high blood pressure, we probably immediately think heart attack, but these are also risk factors for stroke. Further, low physical activity increases the risk for stroke and heart attack. Given that rehabilitation professionals are in the unique position to promote more normal mobility for stroke survivors, but promote health and wellness for the general public to prevent a stroke from happening in the first place. But how do patients know when they are having a stroke?
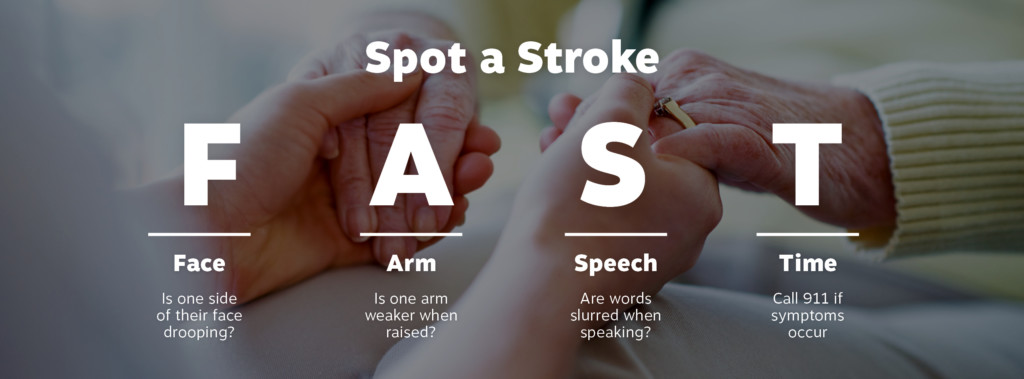
Act FAST: An easy way to remember the signs of stroke is the mnemonic F.A.S.T. , which stands for Facial asymmetry, Arm weakness, Speech problems, and Time-seek medical attention quickly as every minute counts! (Granted, this mnemonic misses some of the less frequently occurring symptoms such as visual problems, vertigo, difficulty walking). For more information on these topics, go to: https://www.cdc.gov/stroke/
Part 2: Rehabilitation tips
Make it measurable. More and more research has identified valid and reliable outcome measures for patients with neurologic deficits. This is not to diminish the value of our observational movement analysis and clinical wisdom, but when we can strengthen our patient’s case with valid, reliable, objective measures, we should. Gait velocity is an example of an outcome measure that can not only define a patient’s current status, but can capture a change in status (improvement or decline), predict frailty in older adults, and is quick and easy to perform. For additional outcome measures, the neurology section of the APTA is an excellent resource for population-specific outcome measures at www.neuropt.org, or go to www.rehabmeasures.org
Practice practice practice. Re-learning how to perform a daily task after a stroke takes practice, and lots of it. Our challenge is to find activities and practice that our patients can do safely when we are not with them- and have the activity be interesting for the patient to want to do it.
Cue outside the body. There a large body of research on attentional focus instructions and motor performance and learning. Originally pioneered by Gabrielle Wulf, simply comparing instructions to focus externally, on an object or aspect in the environment tends to be more effective than having learners focus on body parts. For example, when a patient is standing on a rocker board, “keep the board level” tends to work better than “keep your feet level”. I use this strategy daily- the latest being with a patient with little to no postural control, even with a front wheeled walker. She would stand, then start drifting to the right with absent righting responses, the wheels of the walker lifting off the ground me holding her up. “Keep all four feet of the walker down” got her to correct her loss of balance and she was able to maintain standing for 40 more seconds. Another example is the patient with a tepid performance of a marching exercise, but put a half foam roller above his knee and instruct him to whack it out of your hands and you will find much more speed and engagement than just asking for three sets of 10.
Also, check out my course, “Overcoming Challenges in Stroke Rehab.” Click here to register!
For more information, a great read is: Wulf G, Lewthwaite R, Optimizing performance through intrinsic motivation and attention for learning: The OPTIMAL theory of motor learning. Psychon Bull Rev. 2016 Oct;23(5):1382-1414